Founder of NutriScape.NET. As a dietitian since 1992, Steph Figon has had experiences in consulting, 15 years in clinical, and has operated a private practice nutrition counseling office for since 2011.
Connect on Linkedin
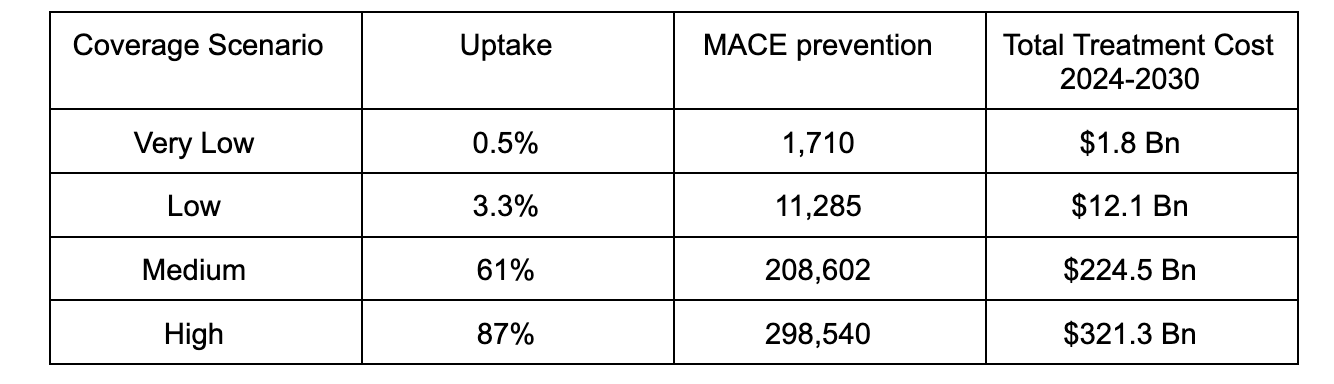
Airfinity analysis on data from the Wegovy trial on cardiovascular outcomes reveals that even after a 65% rebate on the list price, it will cost $1.1m to prevent one heart attack, stroke or cardiovascular death.
If you are thinking about signing up to be a Medicare provider, there are some things to know. This article will boil down some of the most confusing terms, like “par”, “non-par”, “assignment”, and “relative value units”. We’ll cover the limits on what Medicare covers, how you can code it, and where you can provide services. But among the most important is whether Medicare rates will be enough to cover basic business expenses like rent. Read on to find out whether you want to fill out that Medicare Provider Enrollment Form, and the logistical hurdles you’ll encounter if you do.
What Diagnoses Will Medicare Cover?
Medicare only covers Medical Nutrition Therapy (MNT) services for beneficiaries with certain specific diagnoses. These covered diagnoses typically include:
Diabetes: Both Type 1 and Type 2 diabetes are generally covered, reflecting the critical role that diet can play in managing blood sugar levels.
Kidney Disease: This typically includes patients with non-dialysis kidney disease in stages 3-5. MNT can be essential in managing diet to support kidney function.
Post-Kidney Transplant: MNT may also be covered for a certain period following a successful kidney transplant.
That’s it. The thing is that the limitations are hard to get across to your referring providers. This creates a situation where they’ll send referrals for obesity and malnutrition for which these clients have no coverage. This burns up time on your end, but it also affects referrals in subtle ways that aren’t obvious. Namely, the frustration factor for medical providers may affect how willing they are to consider making a dietitian referral at all.
What CPT Codes Does Medicare Consider?
For Medical Nutrition Therapy (MNT) services provided by dietitians, Medicare generally recognizes the following Current Procedural Terminology (CPT) codes:
97802: Medical Nutrition Therapy; initial assessment and intervention, individual, face-to-face with the patient, each 15 minutes.
97803: Re-assessment and intervention, individual, face-to-face with the patient, each 15 minutes.
97804: Group (two or more individuals), each 30 minutes.
How To Look Up The Physician’s Fee Schedule
Step one in the Medicare journey is to establish whether revenue will cover expenses given Medicare’s rates.
Many dietitians find that Medicare rates are not sufficient to support basic business expenses. To look up the rates paid in your area, go to the Physician Fee Schedule. Medicare only recognizes 97802, 97803, and the corresponding group codes.
Relative Value Units: Dietitians Are Paid ??15% Less Than The Physician Fee Schedule
RVUs translate into different reimbursement levels for different types of healthcare providers. Dietitians are generally reimbursed at ??85% of the physician fee schedule for services, meaning that for a service with an established payment rate for physicians, the dietitian would receive 85% of that amount.
So, you might be asking why all the question marks. It’s because the answer was buried so deep in the spreadsheets that it just couldn’t be verified. It appears to depend on your location. Please log in and leave a comment if you know the answer.
Service Locations:
For a time during the pandemic, telehealth was covered under Medicare. Those days are ended, so we’re back in the office, with all the required business expenses offices bring.
For independent dietitians providing Medical Nutrition Therapy (MNT) services to Medicare beneficiaries, reimbursement is available for services provided in these places:
Private Nutrition Offices
Outpatient Clinics: Independent dietitians may offer services in outpatient medical clinics, working in collaboration with other healthcare providers.
Home Health: Independent dietitians may provide MNT services in the patient’s home.
“Par” and “Non-Par”
Medicare, the U.S. federal health insurance program for people aged 65 and older, divides healthcare providers into two main categories: Participating Providers (Par) and Non-Participating Providers (Non-Par). Think of these classifications as being synonymous with “accepting assignment” and “not accepting assignment”.
Participating Providers (Par): Participating providers have signed an agreement with Medicare to accept the Medicare-approved amount as full payment for covered services. This agreement is essentially an agreement to “accept assignment” for all Medicare services provided.
Accepting Assignment: When a provider accepts assignment, they agree to charge only the Medicare-approved amount for a service. Medicare pays Dietitians 100% of this amount, for patients with Diabetes or Stage 3, 4, or 5 Kidney Disease. No other diagnosis is covered, and you basically get 2 hours per year (with some minor exceptions).
Non-Participating Providers (Non-Par): Non-Participating providers can choose to accept or not accept assignment on a case-by-case basis.
Not Accepting Assignment: When a Non-Par provider does not accept assignment, they can charge 15% more than the Medicare-approved amount. There is a limit called the “limiting charge,” which is typically 15% more than the Medicare-approved amount and this can be charged to the patient.
Being a Participating Provider (Par) in Medicare is synonymous with accepting assignment, and this has important implications not only for Medicare billing but also for billing secondary insurance.
The “Limiting Charge” Rule
Medicare Rate (minus the “relative value unit rate) + 15% Is The Max –And It’s Illegal to Charge The Patient More
There is a rule that limits the amount Non-Participating Providers can charge Medicare beneficiaries, known as the “limiting charge.” This rule applies whether or not the patient has secondary insurance.
The limiting charge is typically 15% more than the Medicare-approved amount for the service (though this can vary by state). Here’s how it works:
Medicare-Approved Amount: This is the amount that Medicare has determined is “reasonable” for a particular service. Participating Providers accept this as full payment, while Non-Participating Providers may charge up to the limiting charge of Medicare’s Rate + 15%.
Limiting Charge: For Non-Participating Providers who do not accept assignment, they can charge patients up to 15% more than the Medicare-approved amount. This means they are not accepting the Medicare-approved amount as full payment and are charging the patient up to 15% more.
So, Medicare Non-Participating Providers can charge up to 15% more than the Medicare-approved amount, known as the limiting charge, regardless of whether the patient has secondary insurance.
To Sum It Up
So as you wade into the weeds of considering becoming a Medicare Provider, we hope these details have helped clear up some of the vague concepts and saved you a few hours of time on CMS.gov and on the phone with Medicare representatives, great human beings who seem to answer every question except the one you’re asking.
Learning complex information is hard. When we put things in story form, it’s much easier to learn and remember. NAD+ precursers are at the heart of interventions for fighting age-related diseases and aging itself. A recent research study discusses NAD+ in a rat model of kidney disease and a cell culture.
The Characters
The setting for our main story is the kidney of a diabetic rat. The characters in our story are these:
Mitochondrial Oxidative Stress: Reactive oxygen species, aka free radicals are capable of destroying the energy-producing (ATP-generating) infrastructure in the mitochondria of the nephrons.
NAD+: NAD+ is a critical energy molecule that provides the Sirtuins with their needed fuel.
Sirt3: This is one of seven sirtuin enzymes that alter proteins to manage essential biological processes such as aging and metabolism. By removing acetyl groups from proteins, the process of deacetylation, Sirt3 indirectly influences gene expression, guiding cellular repair functions. Located mainly in the mitochondria, Sirt3 helps regulate energy production and stress response.
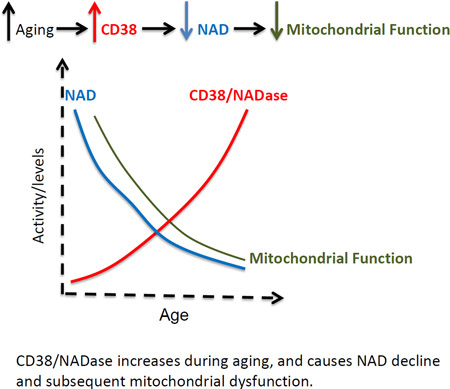
CD38: This is an enzyme that breaks down NAD+, a vital molecule for cellular energy and repair, and its activity is linked to several health conditions such as inflammation and metabolic disorders.
Apigenin: This is a compound in fruits and vegetables that can inhibit CD38, an enzyme that degrades NAD+, thereby improving cell health and fighting inflammation and oxidative stress.
The Story
Once upon a time, in the tiny yet bustling world inside our bodies, there lived a city of countless cells, home to millions of intricate activities. The city’s name was Zucker Diabetic Fatty Rat Kidney, or ZDFRK for short, and it was struggling. A menacing villain known as Mitochondrial Oxidative Stress was causing havoc, contributing significantly to the development of a disease known as diabetic kidney disease, or DKD.
The citizens of ZDFRK knew that a valuable substance, called NAD+, and its diligent partner, the Sirt3 repair protein, were essential to combat the villain. Unfortunately, the levels of NAD+ were dwindling, and Sirt3 repair activity was weakening. This was due to the increasing numbers in the villain army named CD38, notorious for breaking down NAD+.
In the midst of this crisis, a hero emerged from the world of scientific research: Apigenin, a powerful inhibitor of CD38. Apigenin was sent on a mission to rescue the ailing city of ZDFRK. With its CD38 inhibitory powers, Apigenin could potentially restore the balance of NAD+ and Sirt3 and ultimately fight off the nefarious villain, Mitochondrial Oxidative Stress.
In the beginning, Apigenin faced daunting challenges. It found the city of ZDFRK filled with damaged buildings (tubular cells) and filled with a dark cloud of inflammation. But undeterred, Apigenin worked hard, and to everyone’s relief, it significantly reduced these damages. It subdued CD38, restored NAD+ levels, and reignited the activity of Sirt3.
In a parallel universe, a similar city named HK-2, which was also suffering from high glucose levels, saw similar miracles. When Apigenin or CD38 knockdown came to town, they were able to increase NAD+ levels and boost Sirt3 activity.
The success of Apigenin in both cities showed how important CD38 was in the struggle against DKD. By inhibiting Sirt3 and increasing the stress in the city’s mitochondria, CD38 played a significant role in the disease’s development. The heroic actions of Apigenin highlighted the potential of countering CD38 to combat DKD.
And so, the story of Apigenin continues, with hopes of more victories in the fight against diabetic kidney disease. The cells in the cities of ZDFRK and HK-2 will always remember Apigenin, the hero that came to their rescue in a time of crisis.
The Study Described in the Story
In a rat model of kidney disease, researchers studied apigenin, a CD38 inhibitor, to probe the influence of CD38 on diabetic kidney disease (DKD). Researchers noted a significant mitigation in renal injury markers, including tubulointerstitial fibrosis, tubular cellular damage, and the expression of pro-inflammatory genes in diabetic rat models following apigenin administration. In tandem, apigenin treatment also led to a down-regulation in CD38 expression and an upsurge in the intracellular NAD+/NADH ratio and Sirt3-facilitated mitochondrial antioxidative enzyme activity in the diabetic rats’ kidneys.
This fits into what is previously known about DKD. Mitochondrial oxidative stress serves as a pivotal contributor to the onset and progression of DKD. In earlier studies conducted on Zucker diabetic fatty rats, researchers highlighted a correlation between kidney-specific mitochondrial oxidative stress, a diminished intracellular NAD+/NADH ratio, subdued Sirt3 activity, and an escalation in CD38 expression, an enzyme pivotal for NAD+ degradation.
Complementing this, researchers conducted in vitro study that demonstrated an augmentation in the NAD+/NADH ratio and Sirt3 activity in renal proximal tubular HK-2 cells under high-glucose conditions, following either the inhibition of CD38 activity by apigenin or CD38 knockdown.
Collectively, these findings underscore that CD38, by its inhibitory effect on Sirt3 activity and consequent amplification of mitochondrial oxidative stress in renal tubular cells, exerts a critical role in the pathogenesis of DKD. [PMC7343471]
Source: RenueByScience.com/about-apocynin/
Next Steps
No one would argue that animal models are not human trials, and we need human trials to confirm these findings. The problem is that we don’t have them yet and we won’t have them in time to help our clients dealing with kidney disease today. The patient’s decision of whether or not to act on this research will often boil down to an individual’s own very personal risk-reward calculations. But the research itself very clearly indicates that Apigenin can play a beneficial role in the cellular metabolism in diabetic kidney disease.
Educate patients on the risks of using Amazon for supplements: Read this to see some of the reasons it’s just not a trustworthy place to send our patients for supplements. The untrustworthy nature of the entire supplement space was the whole reason why Supplement-Sciences.com was created as a resource for dietitians and our patients. Click the button to find out more.
In the quest to better understand the aging process and potentially slow its relentless march, groundbreaking research by Dr. David Sinclair of Harvard Medical School offers a ray of hope. This article dives into Dr. Sinclair’s intriguing findings on how to restore aged blood vessels with NMN. We explore NMN’s potential role in revitalizing our blood vessels, improving endurance, and perhaps, holding the key to healthier aging.
Of Mice, NMN, and The Vascular Theory of Aging
In a video on the Harvard Medical School site, Dr. David Sinclair explains the effect of NMN on blood vessel regeneration in his research on mice. As we get older, one of the biggest changes that happen in our bodies is that the number of special cells, called endothelial cells that line the inside of our blood vessels, starts to drop. Also, the ones we do have don’t work as well as they used to.
These endothelial cells are super important because they keep our organs and tissues healthy. They do this by making sure we have tiny blood vessels in all the right places. These tiny blood vessels deliver oxygen and nutrients, help control body temperature, and carry away waste products.
The Vascular Theory of Aging
Now, according to a theory called the Vascular Theory of Aging, when these endothelial cells start to fail, it can cause a lot of the problems we usually associate with getting older and can lead to diseases common in old age. In other words, the theory suggests that our blood vessels’ health is a major player in how we age and the diseases we could develop as we get older.
Exercise is currently the best thing we have to slow down the aging effects on these tiny vessels by encouraging the growth of new ones. But, it’s a bit of a mystery why our bodies start to respond less to exercise as we age.
Our muscles are a good place to study this issue because they’re heavily affected by the aging process. As we age, our muscle cells die off more, the growth of new vessels slows down, and there’s an overall loss of blood vessels. This leads to loss of muscle mass and strength and a decrease in stamina in the later years of life, even if we exercise.
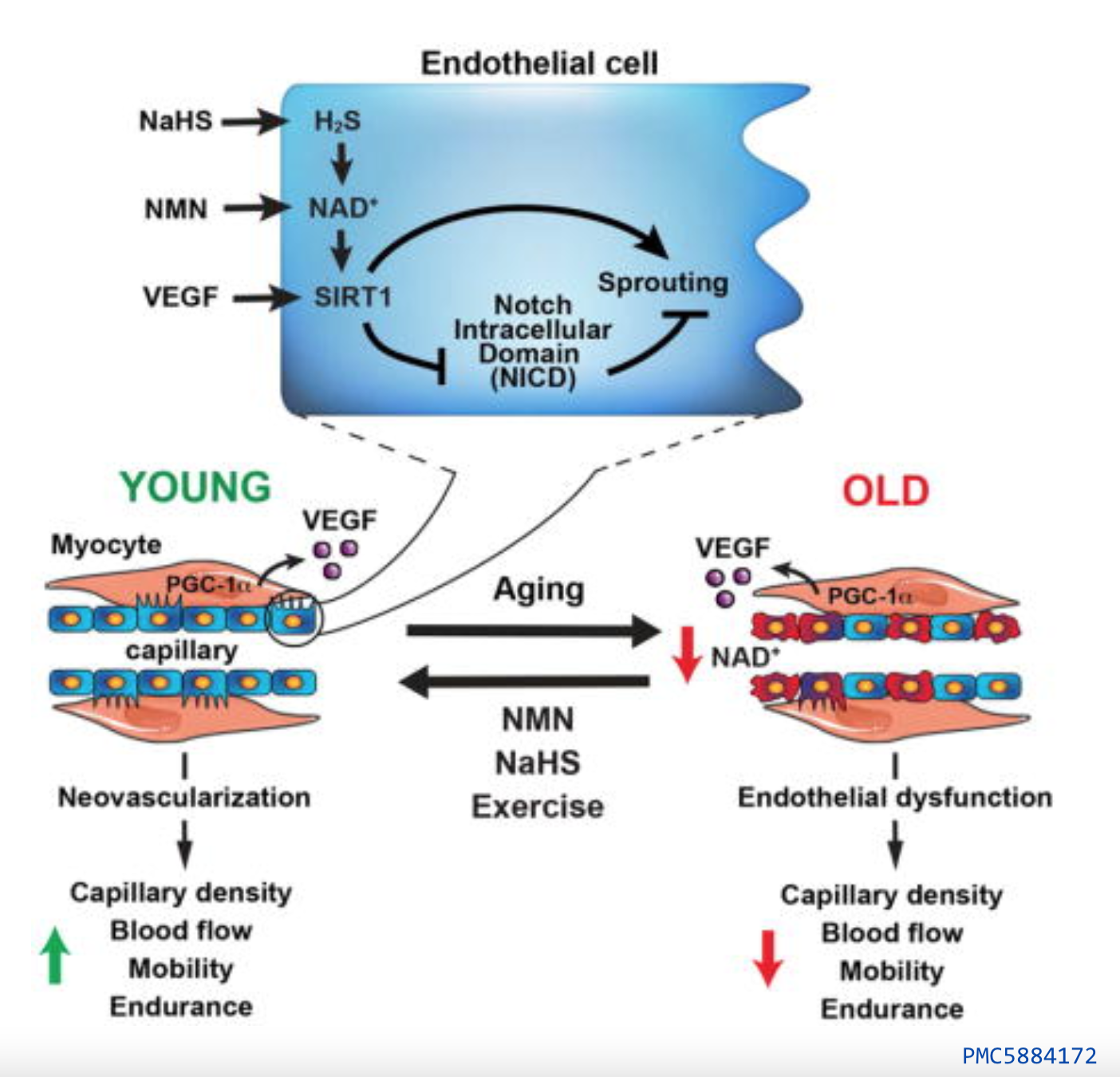
A crucial role in maintaining our health is played by an enzyme in our cells called SIRT1. SIRT1 needs NAD+ to function and is particularly important in our muscles where it helps create new blood vessels. As we age, the activity of SIRT1 may decrease, leading to a reduction in blood flow and stamina.
It Works In Mice–Endurance Up By 56-80%
Sinclair’s study shows that by boosting SIRT1 activity using NMN, we can reverse these aging effects, increase the density of tiny blood vessels in our muscles, and improve exercise ability.
Specifically, NMN treatment managed to bring the number of tiny blood vessels and their density in old mice back to levels usually seen in young mice. It also significantly improved blood flow at rest and oxygen levels in the muscle of treated mice compared to the control group. NMN supplementation noticeably increased oxygen consumption in the mice when they were at rest in their cages, but the most significant effect was a whopping 56–80% improvement in endurance, with lower levels of lactic acid after strenuous exercise after exercise. [PMC5884172]
Although there may be some NMN in various foods, it is tiny compared to the doses used in research studies. And what you can get through food is Vitamin B3 in the form of nicotinamide or nicotinic acid. These forms are nowhere near as effective at raising NAD+ levels as NMN.
First, don’t even think about Amazon for supplements: Read this to see some of the reasons it’s just not a trustworthy place to send our patients for supplements. And, fully acknowledging my own bias, the untrustworthy nature of the entire supplement space with all its half-truths and profit-driven marketing was the whole reason why Supplement-Sciences.com was created as a resource for dietitians and our patients in the first place within the larger context of The NutriScape Project.
But getting back to the specifics of buying NMN supplements on Amazon… ProHealth Longevity (a seller of NMN) published an article in which they discuss their (2020-2021) investigation into adulterated and counterfeit NMN products sold on Amazon.
Their research found that more than half of the NMN products tested contained no NMN at all. Others had less than 80% purity. Some suppliers were selling low-cost vitamin B3 as NMN. Many of these products had fake Certificates of Authenticity and other documentation. Consumer Lab and other parties have now reported similar findings.
Consumer Lab tested the 21 NMN brands with the highest market share on Amazon and found that only three of the brands contained their claimed amounts of NMN. Consumer Lab notes that many of the products that contained virtually no NMN had hundreds or thousands of positive reviews on Amazon. This naturally raises questions about how those reviews were obtained.
The Distinct Flavor That Tells You It Is Real NMN
For trustworthy sources for NMN, check out NMN on Supplement-Sciences.com. Real NMN tastes a little like burnt popcorn and there are only a few suppliers you should trust. This distinct flavor is how I know that I was personally cheated out of about $45 for a bottle of NMN I bought on Amazon… The fake product felt like caffeine and was lemon-flavored and nothing like the flavor of NMN that I am now familiar with. But with such massive potential profits on such an under-regulated platform, who could really expect counterfeiters not to take advantage?
To Sum It Up
Dr. Sinclair’s research points to potential interventions that could slow or even reverse age-related decline. While the complexities of aging are vast, the importance of endothelial health and its relationship to our overall well-being can’t be overlooked. The findings of Sinclair’s study underscore the promising potential of compounds like NMN in boosting the activity of SIRT1, a crucial enzyme in our cells, and promoting the health of our blood vessels. As we continue to unlock the mysteries of aging, NMN emerges as a promising ally in this journey. While there is still much to discover and verify through larger clinical trials, the prospect of enhancing endurance and mitigating the effects of aging through interventions such as NMN supplementation is genuinely exciting. The future of aging research looks brighter than ever, and we are one step closer to transforming the way we age.
Offer courses on general nutrition education or public health topics.
Submit handy food lists of products containing a particular nutrient, the best brands or types of certain foods (i.e. yogurts, protein drinks, breads, and endless other options.) These will be published as “lead magnets” on social media for the purpose of attracting readers to NutriScape.NET and as an incentive to share their email. This enables The NutriScape Project can continue to provide relevant information to readers to promote the dietetic profession.
Submit free or paid downloads for publication on NutriScape.NET.
As registered dietitians, we know exactly what nutrition related labs our clients need and how to interpret nutritional implications for each client. But, to get tested at a lab in the US, a licensed practitioner is required to write a prescription for the individual getting tested. It’s frustrating to our clients that, as dietitians, we can’t get these ordered without putting them through a time-consuming, and unnecessary doctor visit.
Now, Your Clients can Access Nutrition Related Labs
The “supermenu” bar at the very top of the NutriScape.NET site shows a link to the “Labs” page. This direct access to lab results can save your clients time and money while putting you and your client in control with fast results.
Program Features:
You can easily search for the particular lab test(s) your client needs.
Your clients use a simple web login to find a nearby testing center for specimen collection, to place their orders, and to view their results.
A great solution for your cash-pay clients or those with high insurance deductibles. Clients may use their Health Savings Account or Flex Spending Account card to pay for labs. They may also request a coded receipt to submit to insurance. Reimbursement policies will vary by insurance.
Patients don’t need an appointment with their doctor to get the lab results that will help you help them. A remote physician places the lab order electronically for your client immediately. And, if needed, a virtual medical consult is available.
Thousands of lab tests are available at thousands of testing centers in 47 states (excluding NY, RI, and NH).
These presentations do a great job presenting insights into the basic metabolic pathways that nutrition impacts. Understanding the biochemistry of nutrition is something we should all strive to keep up with. Few other free resources present as much content relevant to nutritional biochemistry.
With that said, Dr. Kalish is a chiropractic physician. Also, much of the material is outside our scope of practice, with discussion of herbs and specialized lab ordering. Each dietitian will need to think critically about what is being presented. In other words, The NutriScape Project doesn’t endorse the content.
There are a whole series of similar videos here. Comment below and let us know what you think about the reliability of this content.
 Scan Me!
Scan Me!